It starts innocently enough — a short message from a patient:
“Can I get a refill on my blood pressure meds?”
Quick task, right? Shouldn’t take more than a minute or two.
But if you’re a clinician, you know how the rest of this story goes.
You open the chart. You check the med list. You realize the dose wasn’t updated after their last visit. You skim the last note to confirm your impression. You peek at vitals. You scroll for labs. There’s a flagged potassium from two weeks ago that still needs review. While you’re in the chart, you notice they’re overdue for a follow-up. You wonder if they’ve had their eye exam. Then you go back to the message and try to respond in a way that’s clear, warm, and clinically appropriate — all while watching three more messages roll in.
That “quick” refill? It just cost you 45 minutes. And there are still 17 more waiting in your inbox.
When Did This Become Normal?
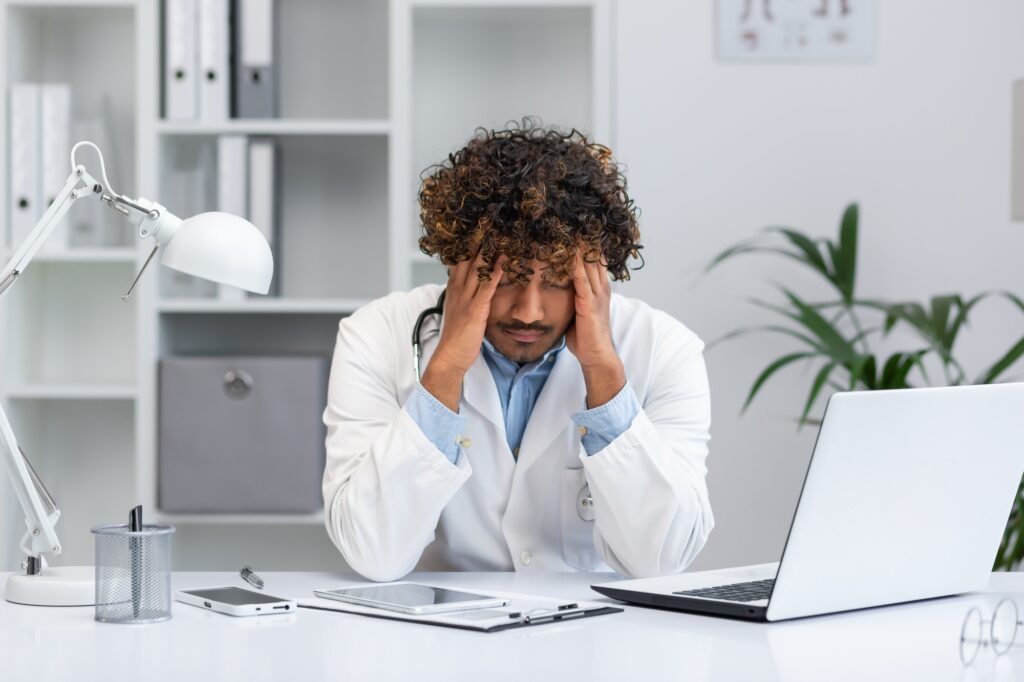
Patient messaging started with the best of intentions. It promised better continuity, faster communication, and more empowered patients. But as these systems scaled, the workload never stopped growing. For many clinicians, what began as a helpful supplement to patient care has now become a second full-time job — one that often starts after dinner.
Inbox work is the new “pajama time.” Quiet, unpaid, untracked — and yet, completely essential to modern care.
The Hidden Weight of the Inbox
The inbox isn’t just where messages go. It’s where decision-making lives:
- Answering a medication question means reviewing meds, labs, allergies, and recent visits.
- Responding to a symptom concern often means triaging a potential acute issue, without the benefit of vital signs or body language.
- Sending a “simple” message back means crafting language that is clinically accurate and understandable to a patient with no medical background.
Every message comes with cognitive load, clinical responsibility, and often, legal documentation. Multiply that by 20–40 messages a day, and you begin to understand why inbox time is one of the fastest-growing contributors to clinician burnout.
Inbox Work Is Clinical Work
We need to stop treating it like a side task. The inbox is a real part of the patient encounter — just without the room, the vitals, or the billing code. Every time a doctor replies to a message, they’re making a clinical decision. But the tools we give them to do this work? Often clunky, inefficient, and completely disconnected from how clinicians think.
When we treat inbox work as invisible, we devalue both the time and the expertise it takes to do it well. And that devaluation — over time — leads to exhaustion, disengagement, and attrition.
What Needs to Change
The inbox isn’t going away. But the way we manage it needs to evolve. We need smarter systems that:
- Draft fast, thoughtful replies for common message types like labs, refills, and routine questions — without starting from scratch.
- Incorporate clinical context — understanding patient history, recent visits, and provider preferences to reduce friction and improve safety.
- Save time without sacrificing empathy — so patients still feel heard, and clinicians aren’t forced to choose between quality and efficiency.
This isn’t about replacing doctors with AI or cutting corners. It’s about respecting their time and supporting the complexity of the work — not making it harder.
We’re Not Asking for Less Work — Just Smarter Work
Clinicians aren’t asking to care less. They’re asking for tools that keep up with the pace and pressure of real practice. Tools that help them respond quickly without burning out. That help them close the loop with patients without spending every evening catching up. That remember their style, their voice, and their standards — and make that easier to deliver, not harder.
Inbox overload doesn’t have to be the norm. But we have to name it, understand it, and design for it — not around it.
Because when the inbox is built smarter, everyone gets better care — including the clinicians behind the screen.